


Do Pro-Life Laws Endanger Women's Lives?
It's helpful for pro-lifers to know this information when confronted with the claim that abortion bans prevent women from receiving care for a miscarriage or an ectopic pregnancy.


It is often claimed by abortion proponents that induced abortions are “coded” the same as many other medical procedures. They also claim that physicians and pharmacists have withheld emergency treatments from patients to avoid any legal gray areas in states where induced abortions are criminalized.
These situations are said to have endangered the lives and safety of patients.
Is there any truth to such claims? To answer that, there are two areas to address: medical coding and delayed treatments.
Medical Coding
The American Academy of Professional Coders (AAPC) defines medical coding as “the transformation of healthcare diagnosis, procedures, medical services, and equipment into universal medical alphanumeric codes.”
The codes are applied to patients’ ongoing records to allow medical professionals to make their expert assessments of conditions and treatments. They are also used to determine the proper reimbursement of services. Medical coding has two components: diagnosis and procedure.
Globally, diagnoses are generally tracked with the World Health Organization’s International Classification of Diseases (ICD) system. Medical professionals in the United States currently use the 10th edition of the Clinical Modifications coding.
This ICD-10-CM system groups the diagnoses by prefixes and numeric values. They can also contain alphanumeric suffixes that act as modifiers.
For purposes of this discussion, obstetric diagnoses come under the heading “Pregnancy, childbirth and the puerperium” with the letter O prefix. They are grouped as follows:
O00-O08 Pregnancy with abortive outcome
O09-O09 Supervision of high-risk pregnancy
O10-O16 Edema, proteinuria, and hypertensive disorders in pregnancy, childbirth, and the puerperium
O20-O29 Other maternal disorders predominantly related to pregnancy
O30-O48 Maternal care related to the fetus and amniotic cavity and possible delivery problems
O60-O77 Complications of labor and delivery
O80-O82 Encounter for Delivery
O85-O92 Complications predominantly related to the puerperium
O94-O9A Other obstetric conditions not elsewhere classified
Drilling down, the subgroup “Pregnancy with abortive outcome” includes:
O00 ectopic pregnancy
O01 hydatidiform mole
O02 other abnormal products of conception
O03 spontaneous abortion
O04 complications following induced termination of pregnancy
O07 failed attempted termination of pregnancy
O08 complications following ectopic or molar pregnancy
Each of these can be modified to provide a clear picture of the diagnosis. For instance, O00 (ectopic pregnancy) has these, among many others:
O00.0 Abdominal pregnancy
O00.1 Tubal pregnancy
O00.2 Ovarian pregnancy
O00.21 Ovarian pregnancy with intrauterine pregnancy
O00.211 Right ovarian pregnancy with intrauterine pregnancy
Clearly, the ICD-10-CM system can be very specific, leaving very little doubt as to the reason for any procedure.
The codes O04 and O07 reference medical conditions relating to previous attempts of induced abortions (called “induced terminations of pregnancy).
However, the diagnosis code for the elective induced abortions themselves actually lies completely outside the scope of obstetrical medical conditions and within the grouping for “Persons encountering health services in circumstances related to reproduction”:
Z30 Encounter for contraceptive management
Z31 Encounter for procreative management
Z32 Encounter for pregnancy test and childbirth and childcare instruction
Z33 Pregnant state
Z34 Encounter for supervision of normal pregnancy
Z36 Encounter for antenatal screening of mother
Z37 Outcome of delivery
Z38 Liveborn infants according to place of birth and type of delivery
Z39 Encounter for maternal postpartum card and examination
Z3A Weeks of gestation
Specifically, Z33 with a modifier:
Z33.2 Encounter for elective termination of pregnancy
This leaves very little doubt as to the reason (i.e. diagnosis) of the induced abortion, so claims of confusion over ectopic pregnancies, miscarriages, etc., are not based on facts. Additionally, medical emergencies under the obstetrics (O) codes and outcomes of delivery (Z37) codes further isolate diagnoses from Z33.2.
The second component of medical coding is the procedure code. In the United States, procedures are tracked with the American Medical Association’s Current Procedure Terminology (CPT) codes and the Centers for Medicare & Medicaid Services’ Healthcare Common Procedure Coding System (HCPCS) codes.
Since HCPCS Level I consists of CPT, we will limit the scope to CPT for this discussion.
The CPT codes are five alphanumeric characters with ranges in consecutive groupings.
Codes for “Maternity Care and Delivery” lie within these ranges:
59000-59076 Antepartum and Fetal Invasive Services
59100-59160 Excision Procedures
59200-59200 Introduction Procedures
59300-59350 Repair Procedures
59400-59430 Vaginal Delivery, Antepartum, and Postpartum Care Procedures
59510-59525 Cesarean Delivery Procedures
59610-59622 Delivery Procedures After Previous Cesarean Delivery
59812-59857 Abortion Procedures
59866-59899 Other Procedures
Procedures of note are:
59100 Hysterotomy, abdominal (e.g. for hydatidiform mole, abortion)
59120-59140 Ectopic pregnancy treatments, surgical
59150-59151 Ectopic pregnancy treatments, laparoscopic
59400-59622 Deliveries (vaginal or Cesarian)
59812 Treatment of incomplete abortion, completed surgically (any trimester)
59820 Treatment of missed abortion, completed surgically (1st trimester)
59821 Treatment of missed abortion, completed surgically (2nd trimester)
59830 Treatment of septic abortion, completed surgically
59840 Induced abortion by dilation and curettage (D&C)
59841 Induced abortion by dilation and evacuation (D&E)
59850 Induced abortion by intra-amniotic injection(s) then delivery
59851 Induced abortion by intra-amniotic injection(s) then D&C or D&E
59852 Induced abortion by intra-amniotic injection(s) thee delivery and hysterotomy
59855 Induced abortion by vaginal suppositories with/without dilation then delivery
59856 Induced abortion by vaginal suppositories with/without dilation then D&C or D&E
59857 Induced abortion by vaginal suppositories with/without dilation then delivery and hysterotomy
59866 Multifetal pregnancy reductions
59870 Uterine evacuation and curettage for hydatidiform mole
The procedure codes for induced abortions, 59840-59857 are clearly separated from other procedures, like those for ectopic pregnancies, miscarriage (i.e. spontaneous abortion) management, molar pregnancies, etc.
Delayed Treatments
If the diagnosis and procedure codes are so explicit in their definitions of induced abortions, is there any validity to claims of delays in treatments that would have been unhindered before recent bans on induced abortions?
Ectopic pregnancies (ICD-10-CM O00):
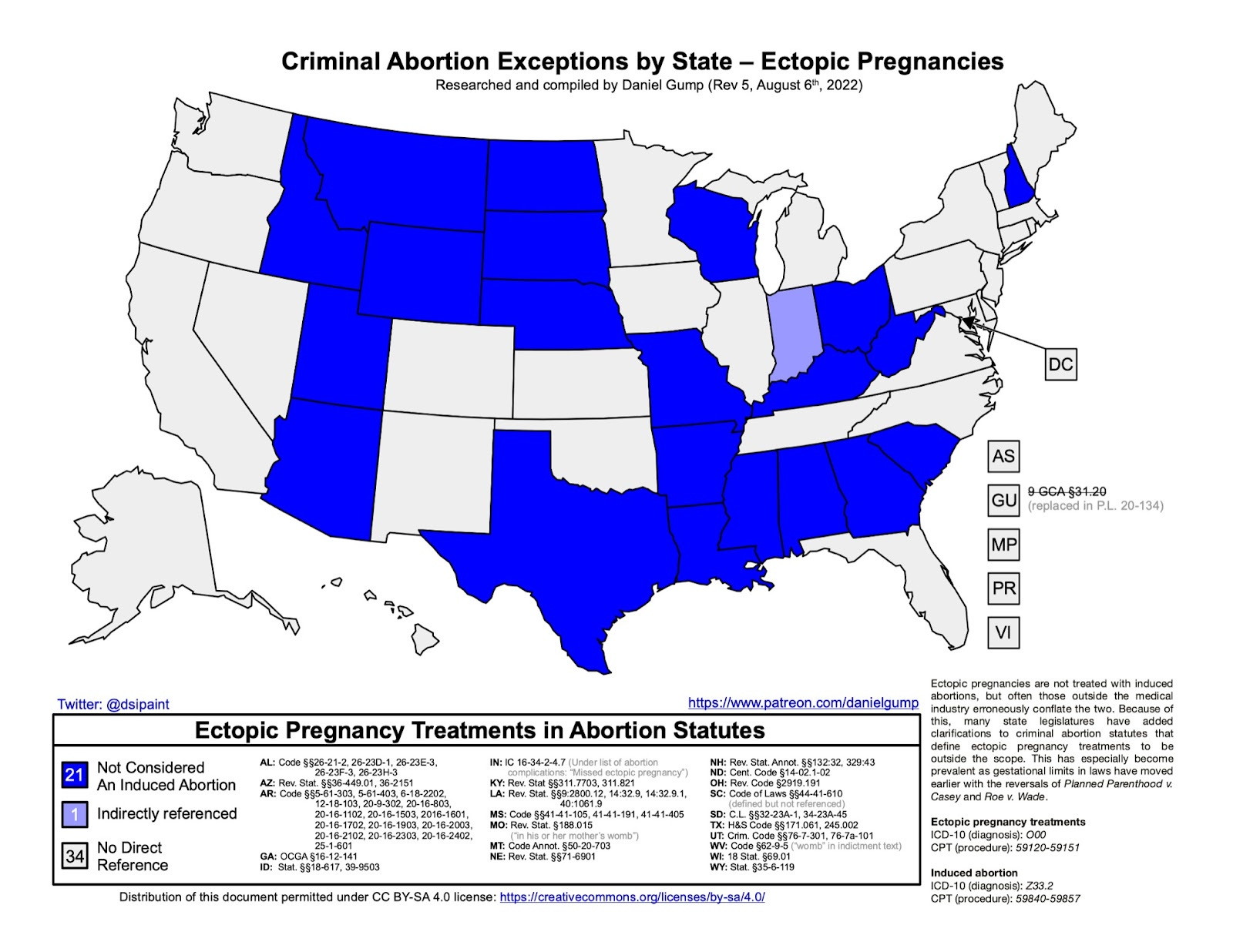
Despite hyperbolic claims to the contrary, not all ectopic pregnancies are emergencies. Patients may be anxious and confused, expecting immediate treatment. Fingers point when treatment is slow.
However, rushed treatments may be more invasive — and even more dangerous — than needed.
Expectant management (i.e. “watching waiting”) is perfectly appropriate for many ectopic pregnancies, as up to 50% of them miscarry naturally with no additional action. Claims have also circulated that pharmacists suddenly started delaying the filling of prescriptions in response to new laws.
However, it has always been important for pharmacists to verify prescriptions before filling them, and that has commonly led to delays in numerous areas. Drugs can interact, elicit allergic reactions, and pose dangers for certain individuals.
For example, methotrexate is used to treat leukemia, severe psoriasis, and rheumatoid arthritis.
It comes with warnings like: “Using this medicine while you are pregnant can harm your unborn baby. The medicine may also cause birth defects if it is used by the father when his sexual partner becomes pregnant.”
Since methotrexate also happens to also be prescribed to treat ectopic pregnancies, it is important for pharmacists to verify the uses before filling prescriptions.
Spontaneous Abortion / Miscarriage (ICD-10-CM O03):
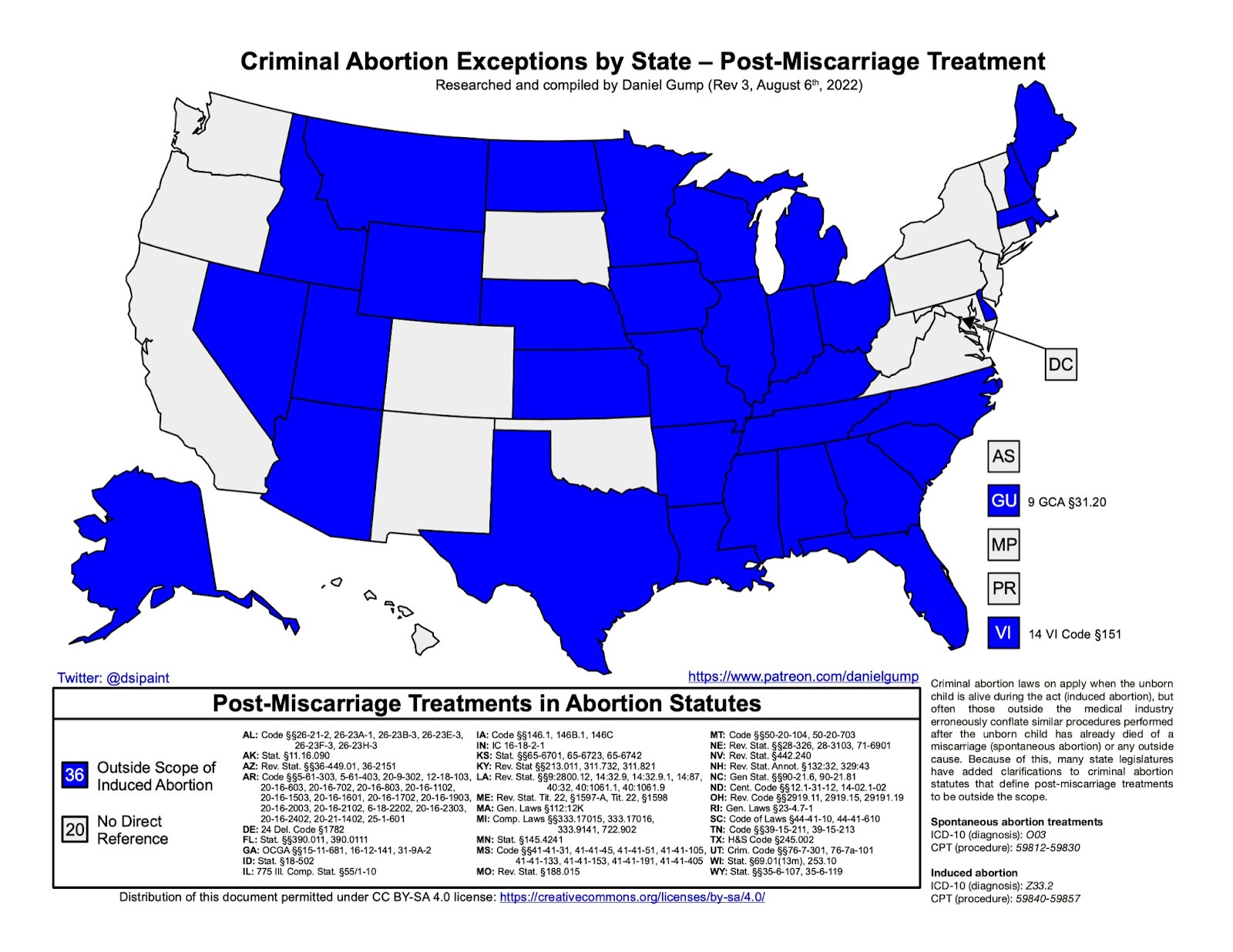
There have also been claims of women being forced to “remain pregnant” after fetal demise. As every criminal abortion law and the CDC’s own definition strictly relate to ongoing intrauterine pregnancies in which the unborn child is alive, these claims can be immediately rejected as outright lies.
Yes, procedures like dilation & curettage are components of both induced abortions and miscarriage management, but claiming they are the same purpose is as absurd as conflating a woman being prescribed Viagra to treat pulmonary hypertension with a man being prescribed it for erectile dysfunction.
As with ectopic pregnancy, miscarriage management may involve a component of expectant management to see if the woman naturally expels the fetal remains.
Medical Emergencies
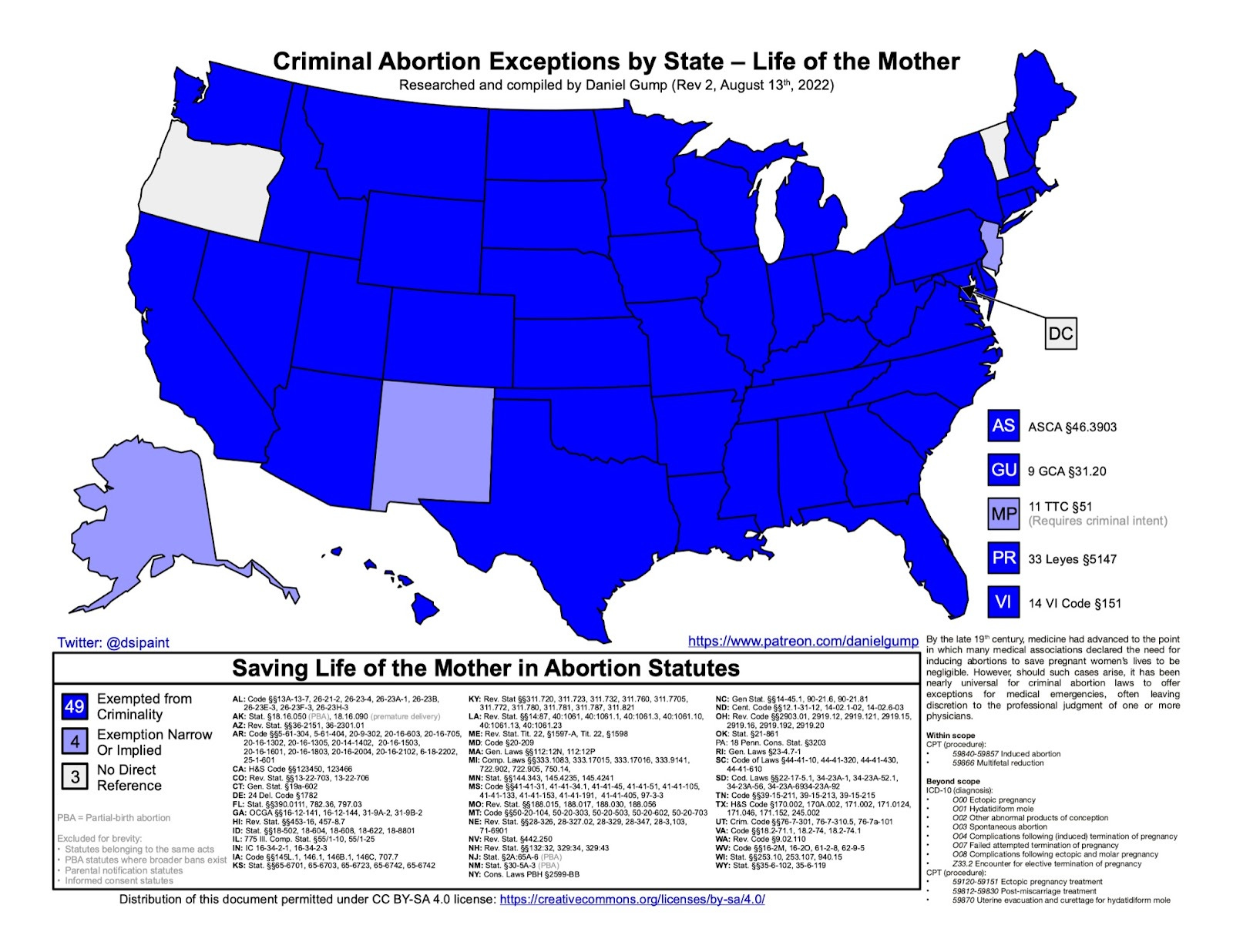
Nowhere in the entire United States is it illegal to perform triage on a pregnant woman, whether or not such treatment results in the death of the unborn child. Anyone claiming such treatment is an induced abortion is either ignorant or is lying.
Be wary of supposed anecdotes on the internet that vaguely claim some unnamed physician at a “Catholic hospital” in some state where induced abortions are banned had to stop emergency treatment to consult an attorney on legalities.
In an emergency, no physician is going to desert a patient to wait for a phone call.
Later in pregnancy, a Caesarian section can be performed in a matter of minutes and is vastly safer than an act of feticide and multiple days of cervical ripening to deliver a dead infant.
Since the CDC's definition of an induced abortion requires that the procedure “does not result in a live birth,” then pre-viability delivery (or preterm parturition) falls outside the scope, as well.
Pro-life OB/GYNs Dr. Poppy Daniels, Dr. C. Brent Boles, Dr. John Bruchalski, and Dr. Christina Francis, have explained this in detail, as has the American Association of Pro-Life Obstetricians and Gynecologists.
If criminal abortion laws are not delaying or preventing critical care from pro-life OB/GYNs, then it brings into question those who are making the claims.
Notice such articles frequently cite abortion providers or representatives of abortion advocacy groups — those who are financially hindered by the laws.
Always follow the money.
 | A guest post by
|